The Elephant In The Room

The evolution of sport science and sports performance has culminated into a data driven culture. Here at SFC we are no different. Our High-Performance Department collects objective data on a multitude of variables. This is done to assess objective metrics and manipulate physical/physiological aspects for improved performance. Our recent blogs have provided some insight on the objective metrics we use to guide our player wellbeing, periodization, and performance. However, this blog will focus more on the psychological aspects of performance (subjective data).
As competitors in a demanding environment our aim is to be stronger and better than our opponents, not showing weakness. Weakness usually being synonymous to our emotions and therefore we attempt to hide them. We get conditioned to not show vulnerability as this could make you an easy target to exploit. In a sports environment we naturally leave psychological matters unaddressed. As coaches and trainers, we are normally unaware of the emotional states of our players.
However, monitoring athlete psycho-social wellbeing is essential to guide training and to detect any progression towards negative health outcomes and associated poor performance1. Mental health and other psycho-social factors have been shown to have a direct effect on player fatigue, readiness to train and subsequently poor performance and increased injury risk. Therefore, it is time to address the elephant in the room…
Having knowledge of player’s psycho-social backgrounds allows us to build relationships and trust as well as an understanding of their needs. Addressing or merely understanding each individuals’ needs allows for better off- and on-field management.
Our first aim at SFC is to carry knowledge of each of our players’ psychometric and social backgrounds. We recognise the value of the information and its effect on performance and injury risk. This information is captured in two questionnaires at the start of each season from each player. The International Olympic Committee’s Sport Mental Health Assessment Tool (SMHAT-1) screens for six different mental health symptoms and disorders. This includes anxiety, depression, sleep disturbance, alcohol misuse, drug use, and disordered eating. The second self-designed questionnaire screens for demographics, for example: place of birth, who raised them, number of dependents, home living conditions, main source of income, academic responsibilities etc.*
Tools such as the SMHAT-1 as well as other curated demographic questionnaires allows the medical staff to have a broader overview of each player’s upbringing, social status, and psychometric wellbeing. This gives a deeper understanding of potential stressors that could contribute to players’ current emotional states. Emotional stress, anxiety, as well as social- and academic responsibilities constitute the subjective (emotional) stress that contributes to the internal workload of the player.
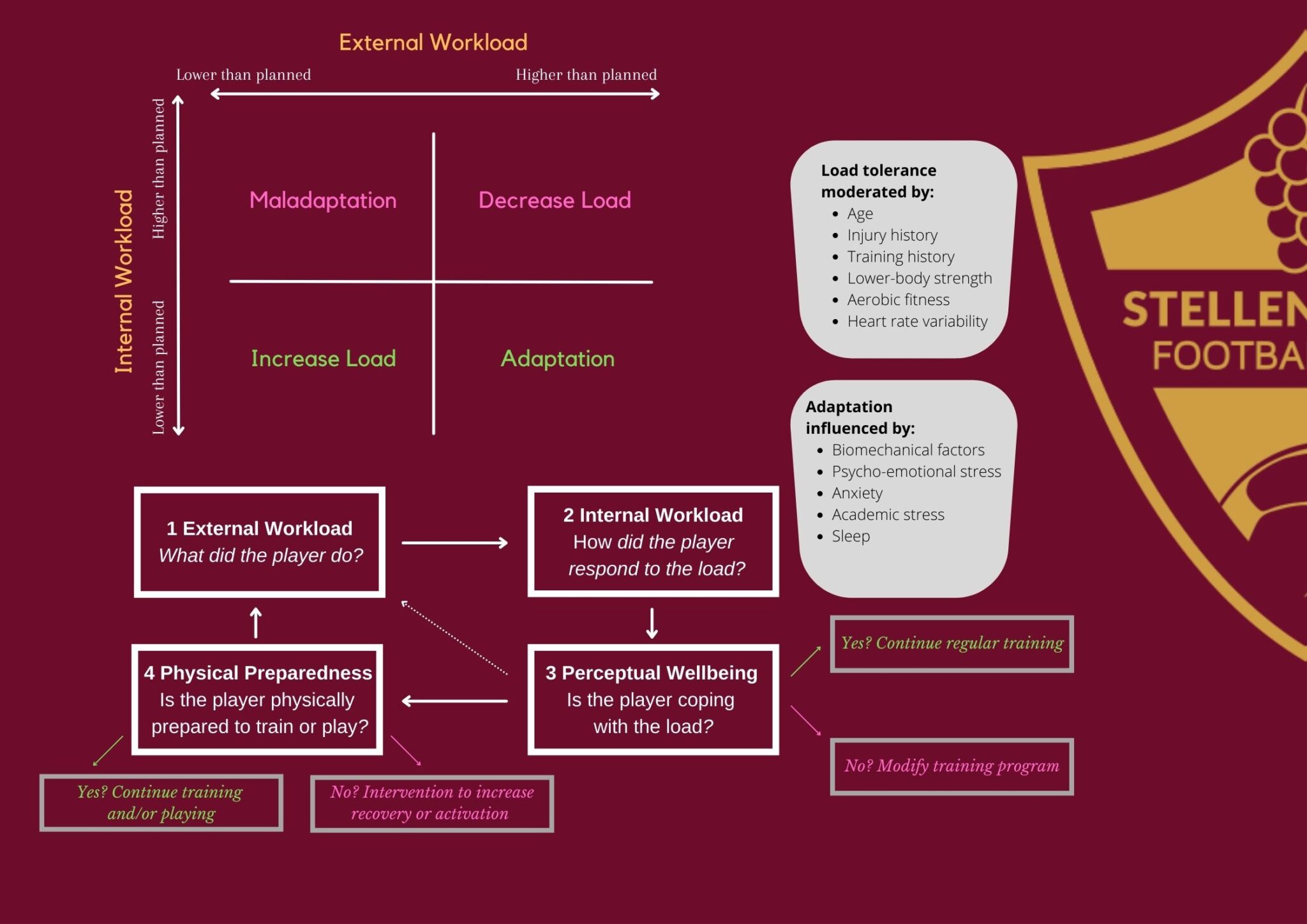
Our second aim at SFC is for our medical staff to be aware of our players acute emotional states. Carrying knowledge of player’s acute emotional states and other subjective wellbeing metrics assists the medical staff to assess training readiness and/or whether a player is adapting to the current loading regime2. In this way external workloads can be altered to aid in recovery and injury risk management.
Unlike the psychometric and social background questionairres, these acute subjective wellbeing metrics is analysed every day in-season. However, it is not easy to talk to each player and their psycho-social wellbeing daily to assess and intervene. Especially when working with a large squad of players as we find in football (25+ players). Sports teams have more recently collected psycho-social wellbeing data in the form of daily questionnaires. Athlete self-reported measures (ASRM) is a relatively simple means for determining a player’s training load and his/her subsequent responses to that training3.
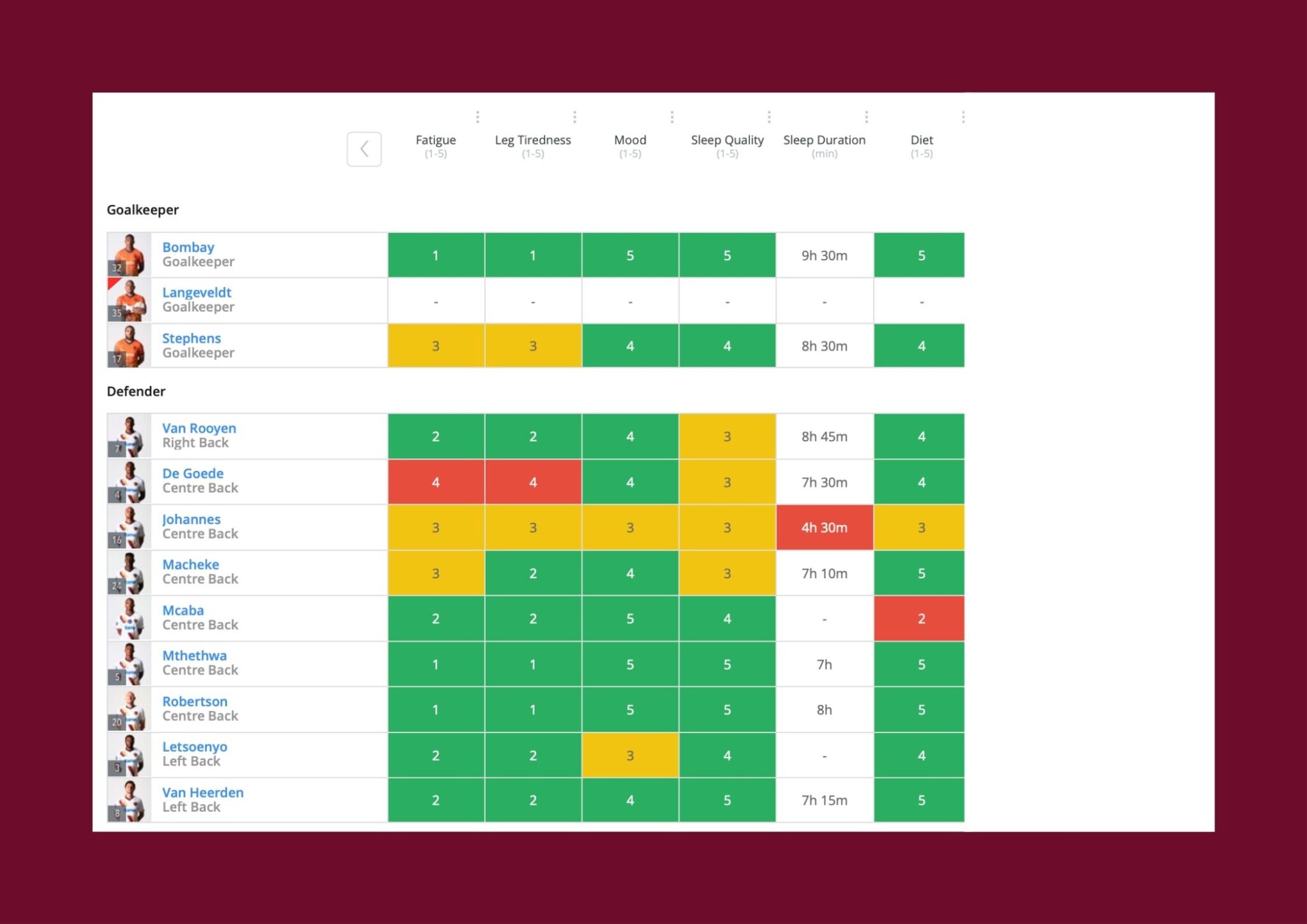
This process is undertaken by the SFC medical and high-performance staff to communicate and plan for the upcoming training session as well as sessions in the micro-plan. We collect daily subjective data on a few variables namely: fatigue, leg tiredness, mood, sleep quality, and diet on a 5-point Likert scale. These metrics then get evaluated each day prior to training to analyse the overall squad or individual outliers for training readiness. This information does not always dictate whether a player trains but rather stimulates a conversation. Why has your sleep been poor? Why are you struggling to keep a good diet? What is affecting your mood? In other words, “real-talk”. Finding solutions or merely understanding problems players would not normally raise in team settings.

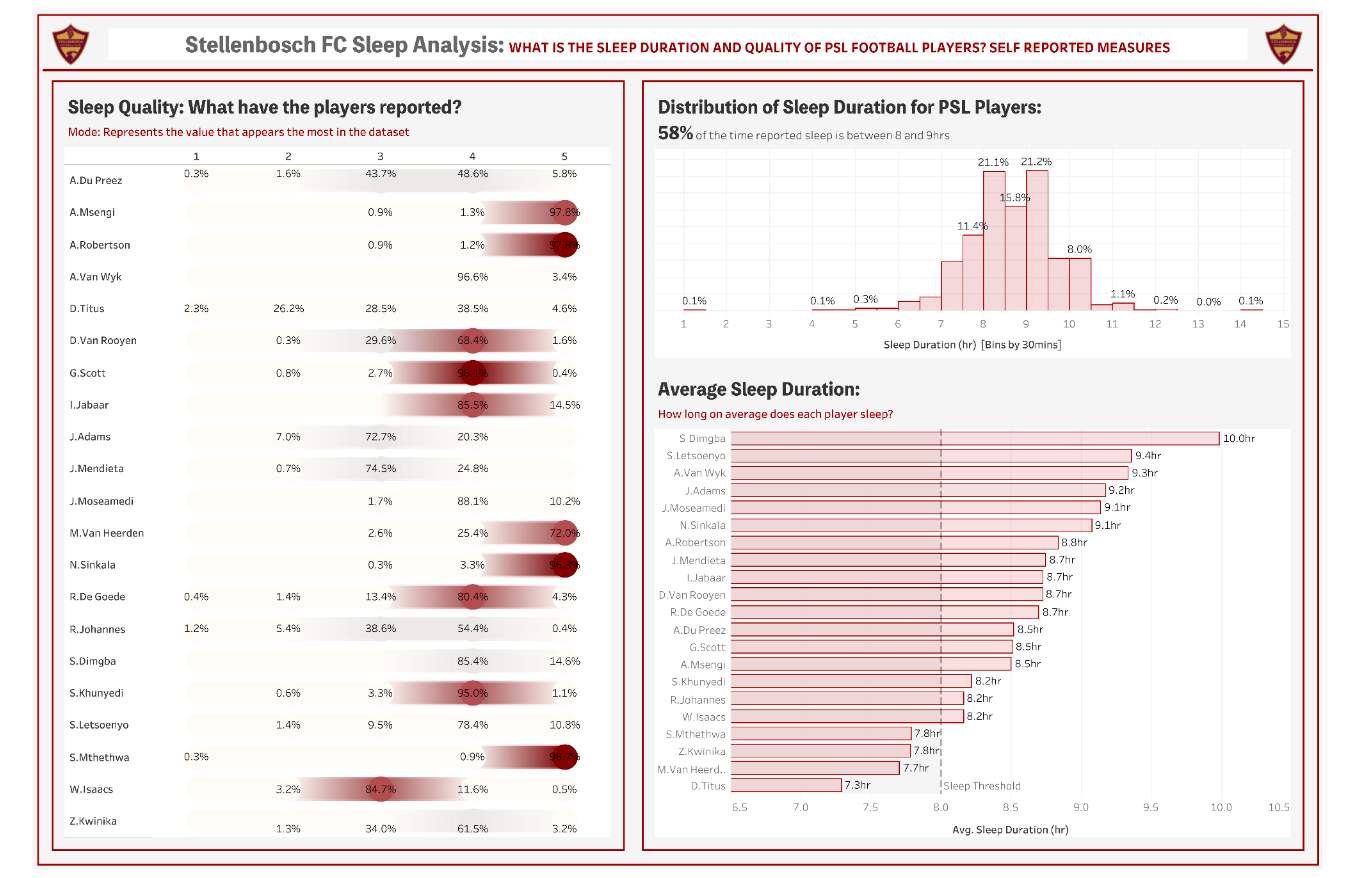
As mentioned before, sports science has recognised the importance of player wellbeing for improved recovery and training readiness. Sleep and nutrition are regarded as the most important aspects of the recovery process4. Here at SFC we have now collected 3 years’ worth of sleep data on our players. We have monitored sleep duration as well as sleep quality daily across this period. Our players sleep between 7-9 hours on average with most reporting their quality of sleep 4 out of 5. This is a good trend according to sleep science5. However, we are more concerned about the data that falls below these parameters. Identifying those individuals with either poor acute or chronic sleep hygiene (duration and/or quality)- which can be addressed to improve player wellbeing.
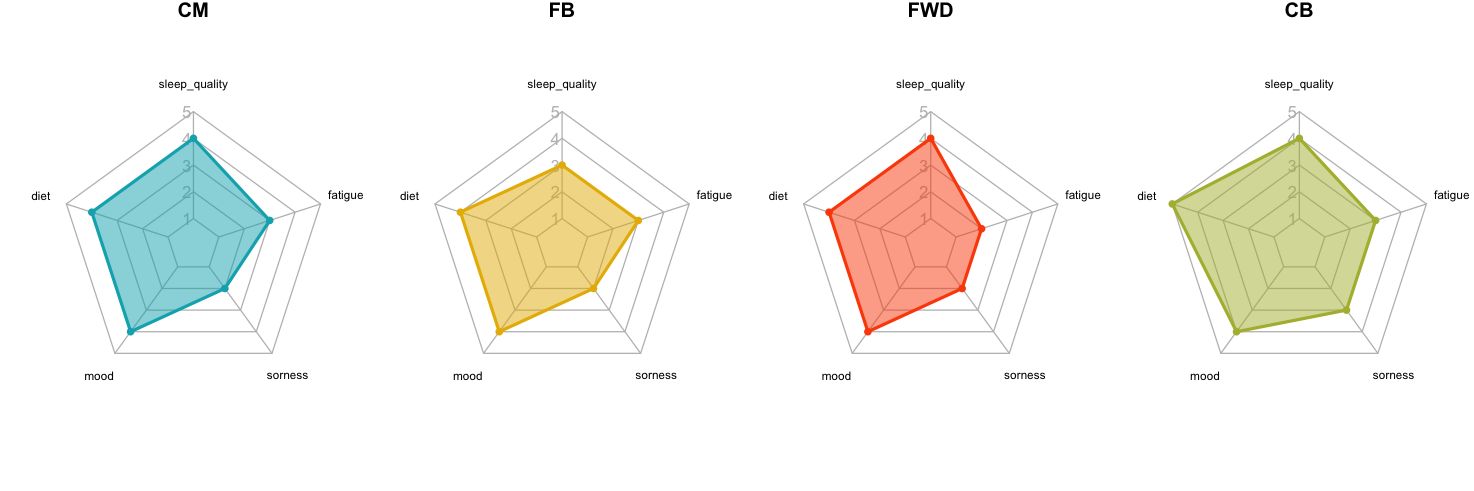
As with sleep, other metrics are also analysed daily. The picture below represents the average score for each subjective metric per player position. Intervention might be required when an individual reports a score different to the group or different to the norm for one or more variables on a specific day. This can stimulate a conversation with the specific individual to potentially adapt the days training and/or spark an intervention to assist in improving those certain aspects of wellbeing. In addition, if most of the group reports values on a specific day that are outside of the norm, then it allows coaches-, conditioning- and medical staff to be aware of high acute or chronic workloads and alter the session volume or intensity to accommodate further regeneration or improvement of subjective wellbeing.
Collecting this subjective data over a long period of time equips our sport science department with more information that could assist with improved session planning and periodization. Using this information longitudinally with the physical output data from GPS monitoring can allow for better decision making on training readiness and acute training outcomes. In other words, when to implement training stressors to allow for adaptation but also when to allow for regeneration for improved subjective wellbeing and ultimately injury or illness prevention.
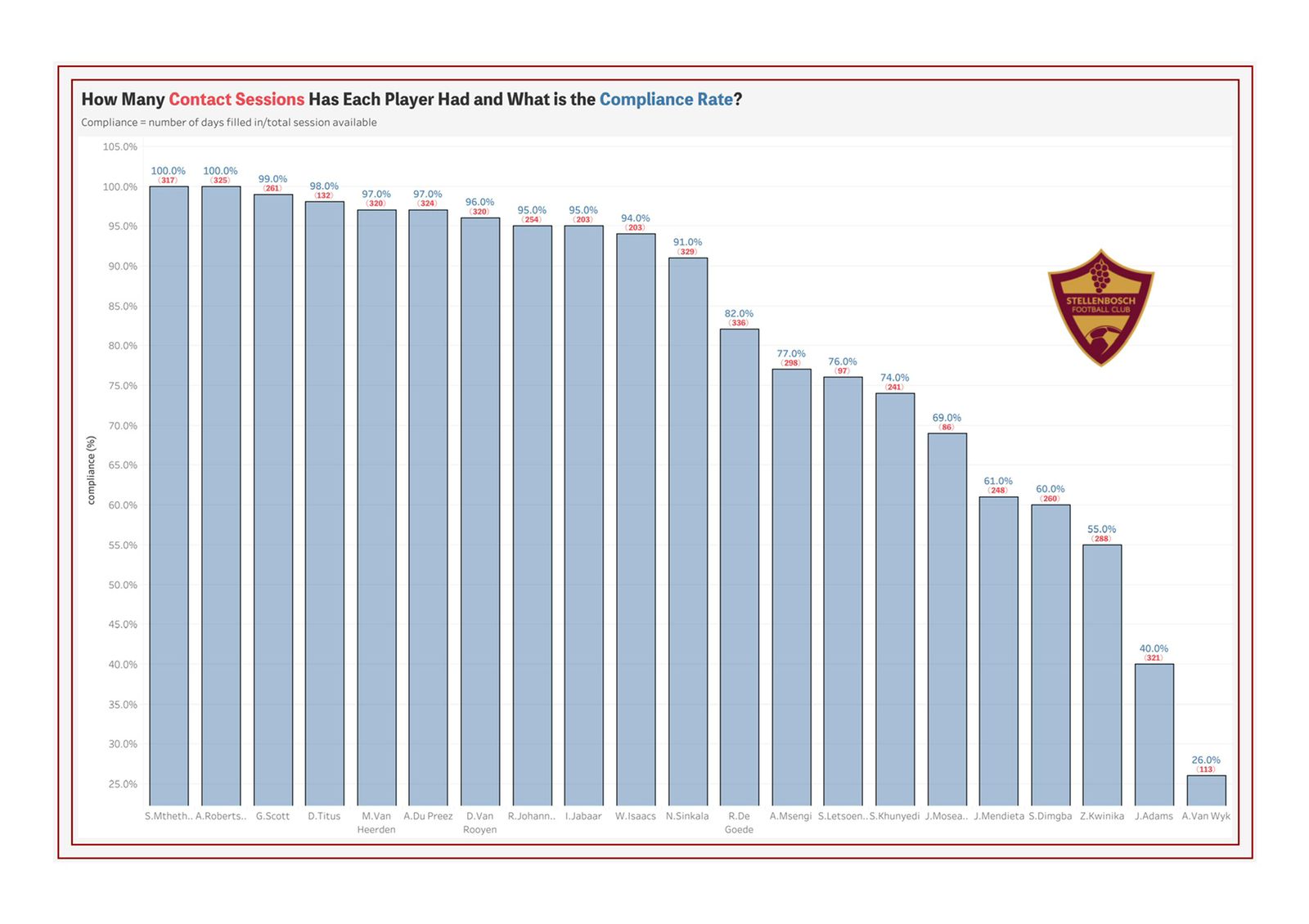
Unfortunately, collecting subjective data is not an automated system but is dependent on human interaction. My experience with subjective data monitoring is 2-fold. For one, player compliance with completing wellness questionairres poses a challenge. The format of collecting data has been simplified to the extent where a player can complete these short questionairres through an app on their smart phones whilst also receiving daily reminder notifications. Regardless, a few players show lack of buy-in or simply forgets to fill in their questionairres consistently. Some also provide untruthful information due to a lack of buy-in and/or understanding.
However, through explanation and education on importance of subjective data collection and monitoring, most players provide useful information to the medical- and performance staff that can be assessed and discussed for improved decision making on periodization and injury risk management.
This brings me to the 2nd part of my experience. It is our role as medical- and performance staff within a sporting environment to educate our players on the importance of psycho-social wellbeing and its relation to performance. Education is our strongest tool as healthcare practitioners and should be utilised as far as possible. Educating our players on sleep hygiene, nutrition and coping mechanisms are only a few of the important aspects worth addressing as found in my own experience. This will hopefully lead to better buy-in to subjective data capturing, more accurate data that can be assessed and ultimately improved psycho-social wellbeing outcomes.
I leave you with a quote: “Caring for the mind is as important as caring for the body. In fact, one cannot be healthy without the other.” ~ Sid Garza-Hillman
*All psycho-social wellbeing information is treated confidentially between the player and medical team and information is only shared with other parties with consent.
References
-
Saw, A. E., Main, L. C., & Gastin, P. B. (2016). Monitoring the athlete training response: subjective self-reported measures trump commonly used objective measures: a systematic review.British journal of sports medicine, 50(5), 281-291.
-
Bourdon, P. C., Cardinale, M., Murray, A., Gastin, P., Kellmann, M., Varley, M. C., … & Cable, N. T. (2017). Monitoring athlete training loads: consensus statement.International journal of sports physiology and performance, 12(s2), S2-161.
-
Saw, A. E., Kellmann, M., Main, L. C., & Gastin, P. B. (2017). Athlete self-report measures in research and practice: considerations for the discerning reader and fastidious practitioner.International journal of sports physiology and performance, 12(s2), S2-127.
-
Halson, S. L. (2008). Nutrition, sleep and recovery.European Journal of sport science, 8(2), 119-126.
-
Merayo, A., Gallego, J. M., Sans, O., Capdevila, L., Iranzo, A., Sugimoto, D., & Rodas, G. (2021). Quantity and quality of sleep in young players of a professional football club.Science and Medicine in Football, 1-6.